CSVS 2025 Antibiogram Report
Goal
Choosing the best single antibiotic, based on evidence, for empiric treatment of Urinary Tract infections pending availability of definitive culture-sensitivity results.
History
Each year, starting in 2022, we construct a yearly antibiogram from urine samples sent to Foundation Laboratory for culture and sensitivity testing when UTI is suspected among our patients. Based on the antibiogram, we select and promote the best antibiotic for immediate initiation of the treatment of presumed UTI while awaiting formal confirmation which takes up to 4 or 5 days. Confirmation leads to either continuation to completion of the erstwhile empiric treatment for the recommended duration of treatment, or a change in regimen to reflect actual findings. This is the report and analysis for 2025, which will inform treatment in 2026.
In 2022 (analyzed early 2023), the best antibiotic was Trimethoprim-Sulfa (TMP/SMZ); in 2023 (applied in 2024), it was Nitrofurantoin; in 2024 (applied in 2025), it was Ciprofloxacin. The following procedure identifies the best antibiotic for empiric treatment of UTI for the year, 2025; the information will be applied the rest of 2026 until we construct another antibiogram in 2027.
Raw Data Source
We obtained culture orders report from Foundation Lab for CSVS patients for the year 2025 for the purpose of constructing an ANTIBIOGRAM.
Exploratory Data Analysis
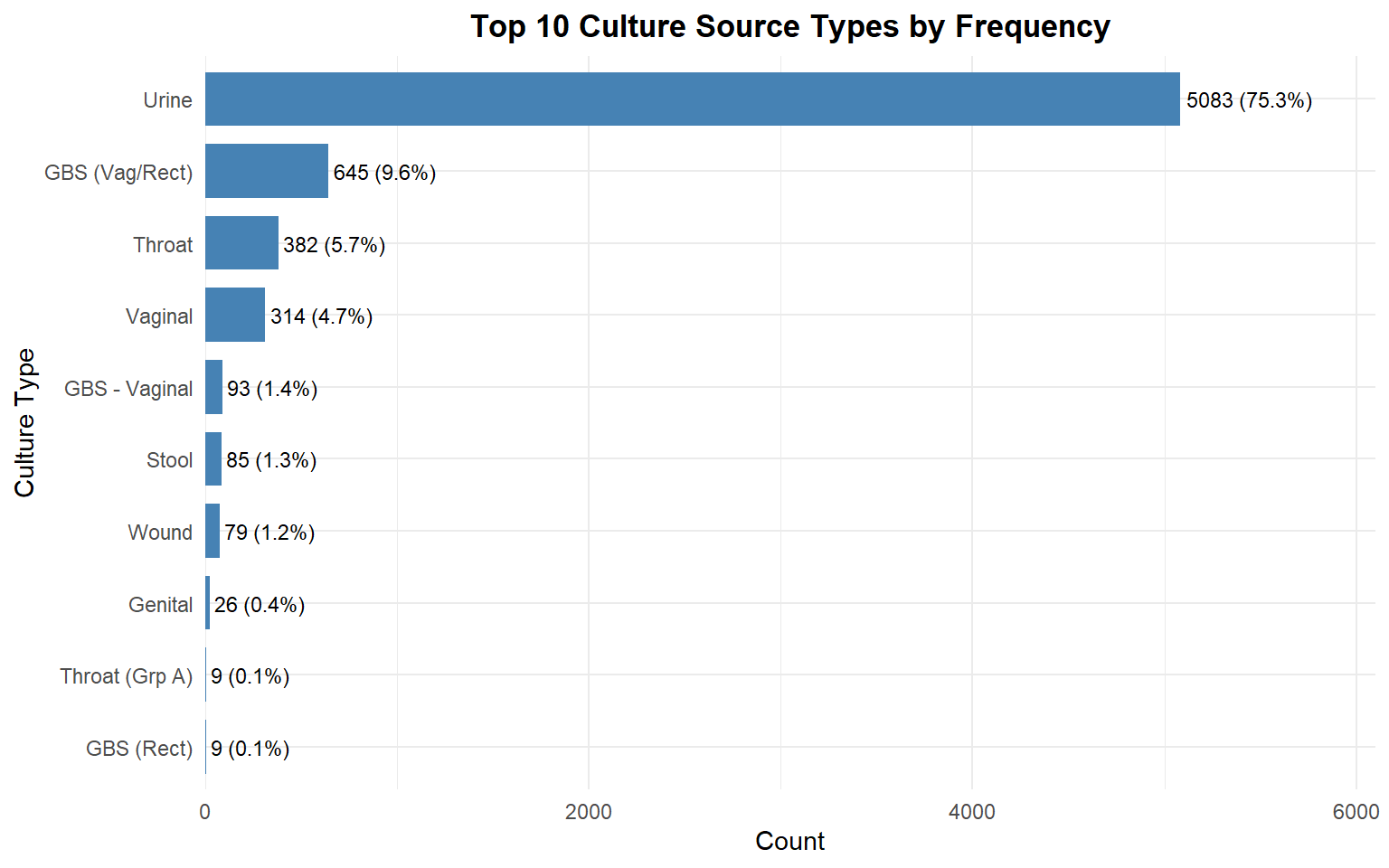
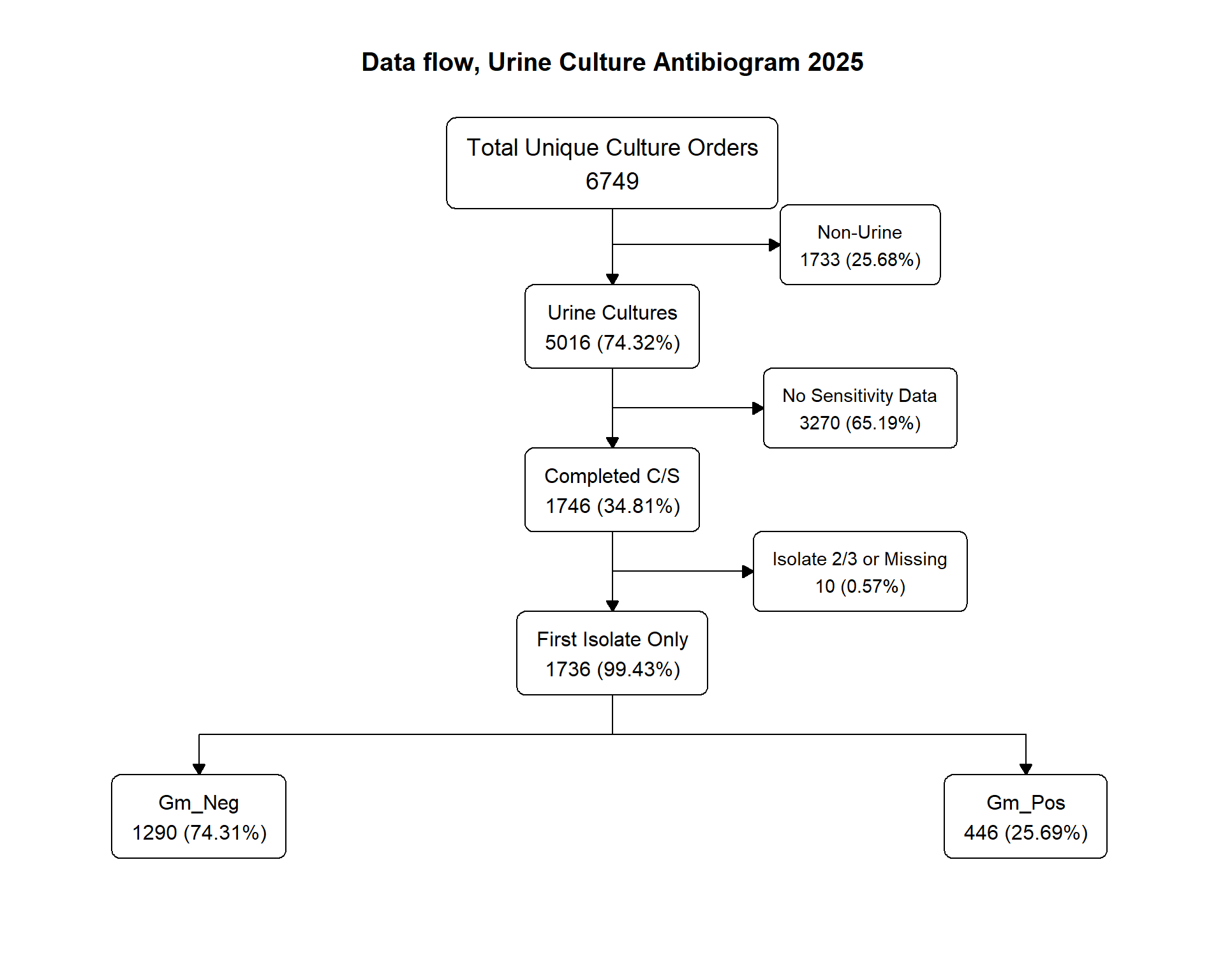
In 2025, CSVS had 6,749 unique specimen culture orders, out of which 5,016 were urine sourced (74.3%). 34.8% (1,746) were acceptable for complete analysis.
Data Pipeline Flowchart
Focusing on the urine cultures, by convention, only the first isolate of a multi-isolate specimen result was counted and used for susceptibility/resistance testing; this subset totalled 1,736 isolates. Here’s the flowsheet for the data processing:
Organism Distribution
Regarding organisms, the chart below shows that Gram-negative E. coli and Gram-positive Enterococcus dominated the isolates list:
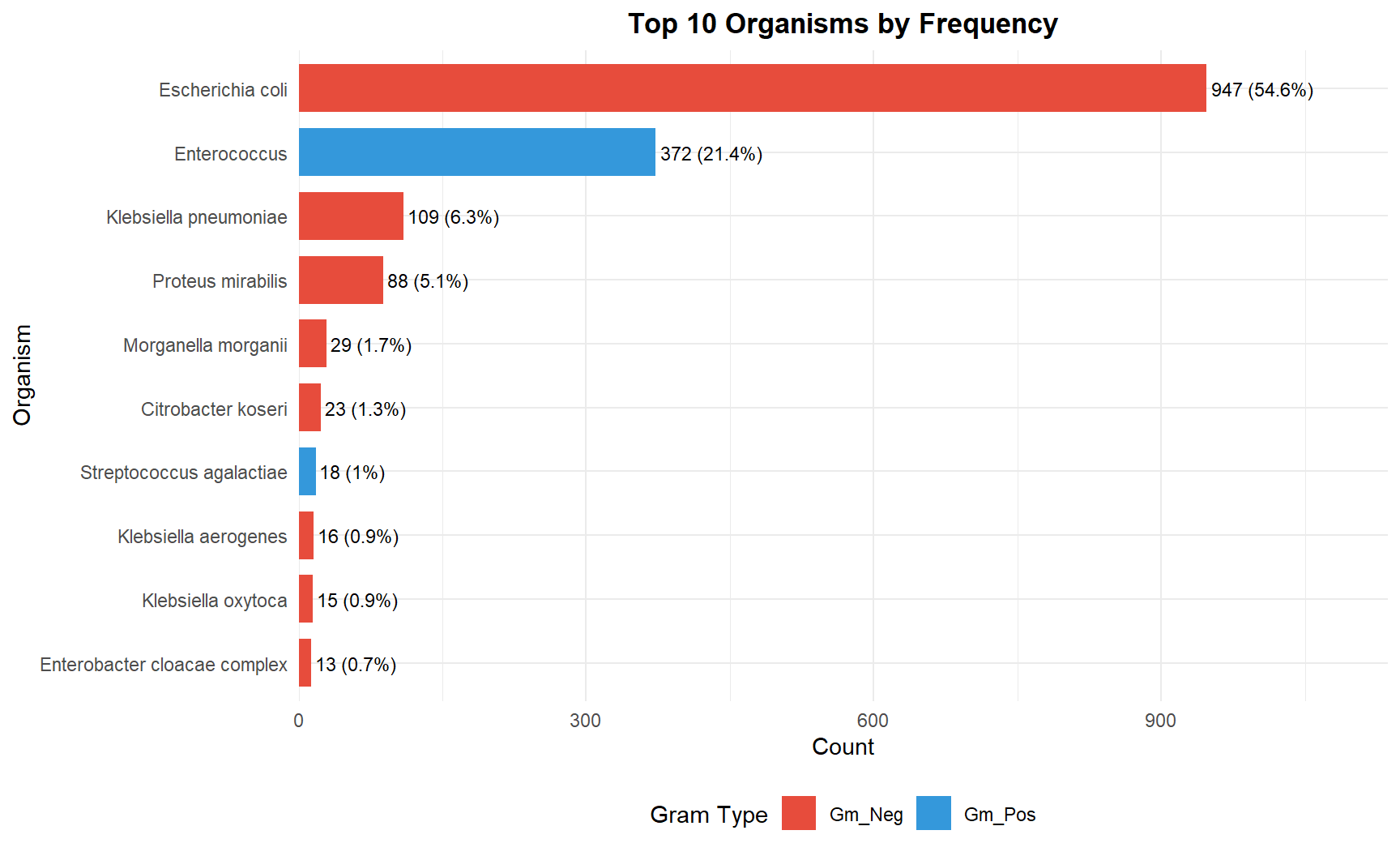
Of 1,736 total isolates:
- 947 (54.6%) were Escherichia coli
- 372 (21.4%) were Enterococcus
Together adding up to 76% of all organisms isolated.
Gram Classification:
- Gram Negative: 1,290 (74.3%)
- Gram Positive: 445 (25.6%)
Antibiogram
The antibiogram below shows the percent susceptibility for each organism-antibiotic combination, calculated directly from the laboratory’s S/I/R (Susceptible/Intermediate/Resistant) interpretations.
| 2025 Antibiogram CSVS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Urine Isolate - Antibiotic Percent Susceptibility Table | |||||||||
| Organism | Gram Type | Isolates | Nitro-furantoin | TMP/SMX | Cipro | Levo-floxacin | Cefazolin | Ceftri-axone | Amp |
| Escherichia coli | Gm_Neg | 947 | 97 | 69 | 63 | 64 | 70 | 90 | 50 |
| Enterococcus | Gm_Pos | 372 | 98 | not tested | 98 | 99 | not tested | not tested | 100 |
| Klebsiella pneumoniae | Gm_Neg | 109 | 30 | 89 | 92 | 93 | 100 | 95 | 0 |
| Proteus mirabilis | Gm_Neg | 88 | 0 | 84 | 94 | 98 | 63 | 99 | 75 |
| Morganella morganii | Gm_Neg | 29 | 0 | 90 | 90 | 93 | 0 | 100 | 0 |
| Citrobacter koseri | Gm_Neg | 23 | 100 | 96 | 96 | 96 | 100 | 96 | not tested |
| Streptococcus agalactiae | Gm_Pos | 18 | not tested | not tested | not tested | 100 | not tested | 100 | 100 |
| Klebsiella aerogenes | Gm_Neg | 16 | 19 | 94 | 94 | 88 | 0 | 88 | not tested |
| Klebsiella oxytoca | Gm_Neg | 15 | 67 | 60 | 87 | 92 | 0 | 73 | 0 |
| Enterobacter cloacae complex | Gm_Neg | 13 | 33 | 92 | 92 | 100 | 0 | 100 | not tested |
| Staphylococcus aureus | Gm_Pos | 12 | 100 | 100 | 83 | not tested | not tested | 100 | not tested |
| Citrobacter freundii | Gm_Neg | 9 | 100 | 100 | 100 | 100 | 0 | 100 | not tested |
| Pseudomonas aeruginosa | Gm_Neg | 9 | not tested | not tested | 100 | 100 | not tested | not tested | not tested |
| Beta Strep Group B | Gm_Pos | 7 | 100 | 100 | 71 | 67 | 67 | 100 | 67 |
| Coagulase negative Staphylococcus | Gm_Pos | 7 | 100 | 100 | 86 | not tested | not tested | 50 | not tested |
Interpretation
Escherichia coli (54.6%), Enterococcus (21.4%), Klebsiella pneumoniae (6.3%), Proteus mirabilis (5.1%), Morganella morganii (1.7%) and Citrobacter koseri (1.3%) make up 90% of UTI organisms.
Nitrofurantoin, Levofloxacin and Ciprofloxacin are the top and equal contenders for the best choice of empiric antibiotics for UTI organisms
Ciprofloxacin provides good coverage for the most common organisms consistently >= 90%, except against E.coli—by far the most common isolate—where susceptibility is a paltry 63%. Levofloxacin shares Ciprofloxacin’s profile while besting it by a few percentage points consistently. By comparison, Nitrofurantoin covers 97% of E.coli. It also has great coverage (98%) for the next most common isolate, gram positive Enterococcus (same as Cipro, 98%; 99% for Levofloxacin). However, Nitrofurantoin has very poor coverage for Klebsiella, Proteus and Morganella, if at all.
Ceftriaxone is also effective, (not active against Enterococcus) but it is parenterally administered (available on CSVS in-house Formulary for IM injection). Effectiveness does not carry over to oral cephalosporins.
Cefazolin, the oral cephalosporin tested, mirrors the profile of Ceftrioxone, but much less coverage for E.coli, Proteus and Morganella; more for Klebsiella and Citrobacter.
TMP/SMX has limited effect on Enterococcus and other Gram-positive organisms but coverage is fairly good for other isolates.
Ampicillin covers Gram-positive organisms well (100%) but has very limited limited Gram-negative coverage. This would constitute an inadequate choice for empiric antibiotic UTI treatment.
Summary
“All things being equal…”, for empiric UTI treatment pending culture results:
- First choice: (3-way tie)
- Nitrofurantoin (comes as MacroBID for BID dosing), if basing decision on sheer numbers alone.
- Levofloxacin, if basing decision on broadness of effectiveness; also has good tissue penetration.
- Ciprofloxacin—same as Levofloxacin—if basing decision on broadness.
- Fourth choice: (2-way tie)
- Cefazolin (has good tissue penetration)
- TMP/SMX
- Not Recommended:
- Ampicillin
BTW: Fosfomycin (for UTI, a single dose regimen) was not tested; efficacy and safety profile favors its use in pregnancy. We worked with MediCal / Medicaid earlier to place it on their formulary
Caveat
- Always obtain UA if thinking of, or ruling out, UTI/Cystitis
- Obtain culture/sensitivity:
- If any abnormality in Nitrites, Heme or Leuko; or
- If planning to treat
- Susceptibility patterns do not necessarily carry over to other members of an antibiotic class
- The profile in the table above is specific to the named antibiotic, and is not an antibiotic class property
- Fosfomycin (single dose for UTI) [Culture-Sensitivity not run] is guideline-acceptable treatment in all pregnancy trimesters; it is now on MediCal / Medicaid formulary