CSVS 2024 Antibiogram Report
Goal:
Choosing the best single antibiotic, based on evidence, for empiric treatment of infections pending availability of definitive culture-sensitivity results.
History:
Each year, starting in 2022, we construct a yearly antibiogram from urine samples sent to Foundation Laboratory for culture and sensitivity testing when UTI is suspected among our patients. Based on the antibiogram, we select and promote the best antibiotic for immediate initiation of the treatment of presumed UTI while awaiting formal confirmation which takes up to 3 to 5 days. Confirmation leads to either continuation to completion of the erstwhile empiric treatment for the recommended duration of treatment, or a change in regimen to reflect actual findings. This is the report and analysis for 2024, which will inform treatment in 2025.
In 2022 (analyzed early 2023), the best antibiotic was Trimethoprim-Sulfa (TMP/SMZ); in 2023 (applied in 2024), it was Nitrofurantoin. The following procedure identifies the best antibiotic for empiric treatment of UTI for the year, 2024; the information will be applied the rest of 2025 until we will construct another antibiogram in 2026.
Raw Data Source:
We obtained culture orders report from Foundation Lab for CSVS patients for the year 2024 for the purpose of constructing an ANTIBIOGRAM.
EXPLORATORY DATA ANALYSIS
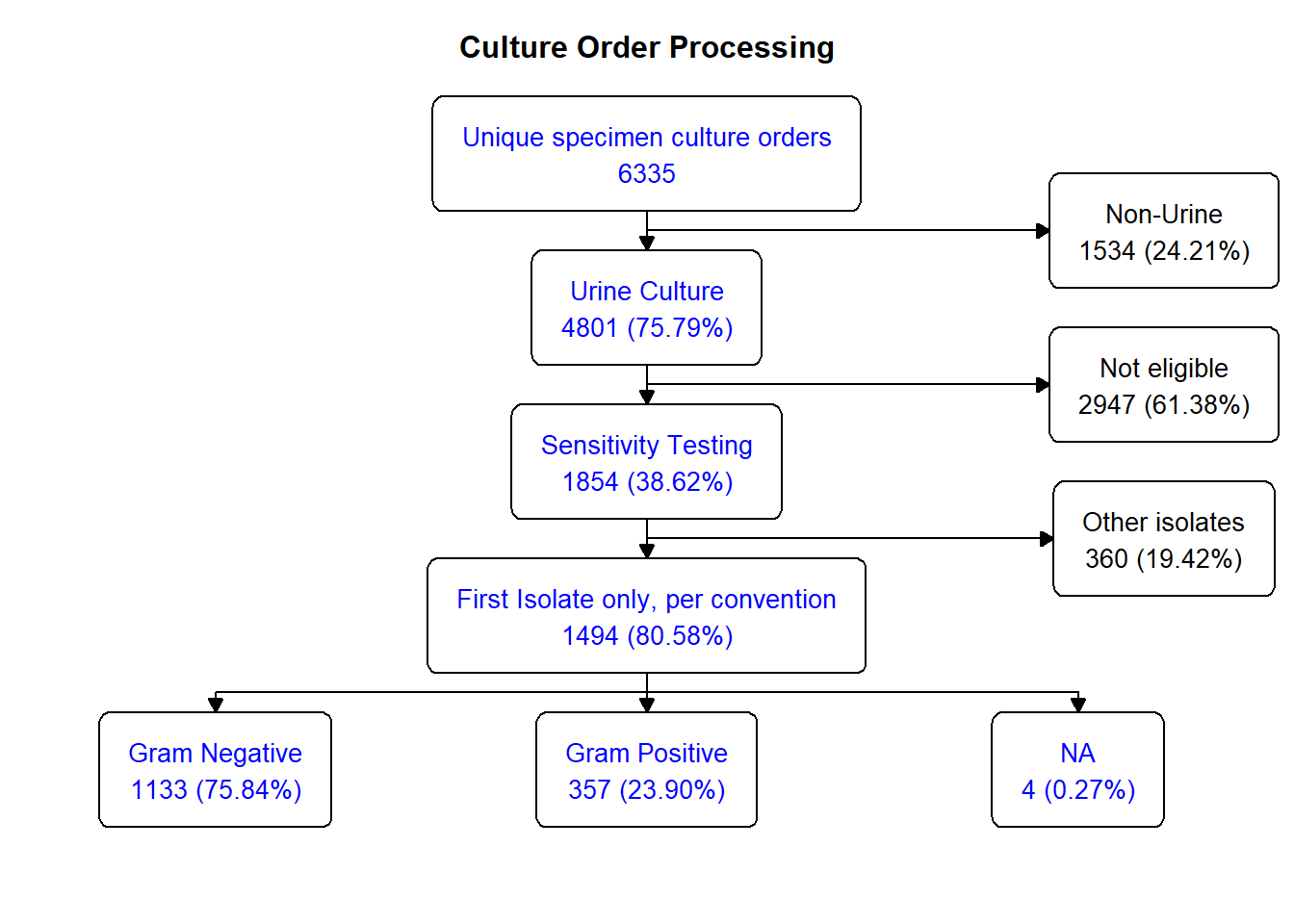
In 2024, CSVS had 6335 unique specimen culture orders, out of which 4801 were urine sourced (75.8%). 38.6% (1854) were acceptable for complete analysis. Here’s the breakdown:
Focusing on the urine cultures, by convention, only the first isolate of a multi-isolate specimen result was counted and used for susceptibility / resistance testing; this subset totalled 1494, yielding 31.1% of all cultured urine specimen – a little under a third . Here’s the flowsheet for the rest of the process:
Regarding organisms, the chart below shows that gram neg E coli and gram pos Enterococcus spp dominated the isolates list:
Of 1494 total isolates,
- 865 or 58% were Escherichia coli
- 281 or 18.8% were Enterococcus sp.,
together adding up to 77% of all organisms isolated.
Antibiogram
Using the global application tool, WHONET and it’s companion program, BacLink, the dataset from above was mapped and standardized to produce the universal antibiogram-related reports. From the reports, the following output was created…
| 2024 Antibiogram CSVS | |||||||||
| Urine Isolate - Antibiotic Percent Susceptibility Table | |||||||||
| Organism | Gram Type | nbr of isolates | Nitro-furantoin | TMP/SMX | Cipro | Levo-Floxacin | Cepha-zolin | Ceftri-oxone | Amp |
|---|---|---|---|---|---|---|---|---|---|
| Escherichia coli | Gram Negative | 865 | 100 | 99.8 | 100 | 0.2 | 100 | 100 | 0 |
| Enterococcus sp. | Gram Positive | 281 | 100 | 100 | 100 | 100 | 100 | 100 | |
| Klebsiella pneumoniae ss. pneumoniae | Gram Negative | 82 | 0 | 100 | 100 | 100 | 100 | 100 | 0 |
| Proteus mirabilis | Gram Negative | 62 | 0 | 100 | 100 | 100 | 100 | 100 | 0 |
| Streptococcus agalactiae | Gram Positive | 44 | 100 | 100 | 100 | 100 | 100 | ||
| Morganella morganii ss. morganii | Gram Negative | 26 | 0 | 7.7 | 23.1 | 23.1 | 0 | 100 | 0 |
| Klebsiella oxytoca | Gram Negative | 20 | 100 | 0 | 100 | 100 | 0 | 0 | 0 |
| Citrobacter koseri | Gram Negative | 15 | 100 | 100 | 100 | 100 | 100 | 100 | |
| Klebsiella aerogenes | Gram Negative | 14 | 100 | 100 | 100 | 100 | 0 | 100 | |
| Staphylococcus aureus ss. aureus | Gram Positive | 14 | 100 | 85.7 | 85.7 | ||||
| Serratia marcescens | Gram Negative | 10 | 0 | 100 | 100 | 100 | 0 | 100 | |
| Enterobacter cloacae | Gram Negative | 9 | 11.1 | 100 | 100 | 100 | 0 | 88.9 | |
| Pseudomonas aeruginosa | Gram Negative | 8 | 100 | 100 | 100 | ||||
| Raoultella ornithinolytica | Gram Negative | 7 | 100 | 100 | 100 | 100 | 0 | 100 | 0 |
| Citrobacter freundii | Gram Negative | 6 | 100 | 100 | 100 | 100 | 0 | 100 | |
| Staphylococcus epidermidis | Gram Positive | 4 | 100 | 100 | 100 | ||||
| Raoultella planticola | Gram Negative | 2 | 100 | 100 | 100 | 100 | 100 | 100 | 0 |
| Enterococcus faecium | Gram Positive | 2 | 100 | 100 | 0 | ||||
| Streptococcus gallolyticus ss. gallolyticus | Gram Positive | 2 | 100 | 100 | |||||
| Staphylococcus haemolyticus | Gram Positive | 2 | 100 | 100 | 100 | ||||
| Streptococcus sp. | Gram Positive | 2 | 100 | 100 | |||||
| Streptococcus viridans, alpha-hem. | Gram Positive | 2 | 100 | 100 | |||||
| Rhizobium radiobacter | Gram Negative | 1 | 0 | 0 | 100 | 100 | |||
| Pantoea sp. | Gram Negative | 1 | 100 | 100 | 100 | 100 | 100 | ||
| Stenotrophomonas maltophilia | Gram Negative | 1 | 100 | 100 | |||||
| Proteus vulgaris | Gram Negative | 1 | 0 | 100 | 100 | 100 | 0 | 100 | 0 |
| Serratia liquefaciens | Gram Negative | 1 | 0 | 100 | 100 | 100 | 0 | 100 | |
| Serratia odorifera | Gram Negative | 1 | 0 | 100 | 100 | 100 | 0 | 100 | |
| Serratia plymuthica | Gram Negative | 1 | 0 | 100 | 100 | 100 | 0 | 100 | |
| Enterococcus faecalis | Gram Positive | 1 | 100 | 100 | 100 | ||||
| Streptococcus anginosus | Gram Positive | 1 | 100 | 100 | |||||
| Staphylococcus, coagulase negative | Gram Positive | 1 | 100 | 100 | 0 | ||||
| Staphylococcus lentus | Gram Positive | 1 | 100 | 100 | |||||
| Staphylococcus simulans | Gram Positive | 1 | 100 | 100 | 100 | ||||
| Staphylococcus sp. | Gram Positive | 1 | 100 | 100 | 0 | 100 | 100 | 100 | |
Interpretation
E coli (58%), Enteroccoccus sp. (19%), Klebsiella pn. (6%), Proteus m. (4%) and Strep ag. (3%) make up almost 90% of UTI organisms;
Cipro provides the best coverage for those organisms and is oral.
- Cipro provides the best coverage for all the organisms tested.
Ceftrioxone is just as good, but it is parenterally administered (available on CSVS Formulary for IM injection). Effectiveness does not carry over to oral cephalosporins
Nitrofurantoin is the next best antibiotic, missing Klebsiella and Proteus; followed by
SMX/TMP, which has no effect on Enterococcus and other gram positive organisms
Ampicillin covers only gram positive organisms (24% of isolates), and Gram negative Pseudomonas, an insignificant (by numbers) cause of UTI. This would constitute an inadequate choice for empiric antibiotic UTI treatment
Summary
“All things being equal…”, for empiric UTI treatment pending culture results:
- First choice:
- Cipro
- Second choice:
- Nitrofurantoin (comes as MacroBID for BID dosing)
- Third choice:
- TMP/SMX
- Levaquin
- Not Recommended:
- Ampicillin
BTW: Fosfomycin (for UTI, a single dose regimen) was not tested; efficacy and safety profile favors its use in pregnancy
Caveat:
- Always obtain UA if thinking of, or ruling out UTI / Cystitis;
- Obtain culture / sensitivity
- if any abnormality in Nitrites, Heme or Leuko; or
- if planning to treat.
- Susceptibility patterns do not necessarily carry over to other members of an antibiotic class
- The profile in the table above is specific to the named antibiotic, and is not an antibiotic class property
- Fosfomycin (single dose for UTI) [Culture-Sensitivity not run, as above] is guideline-acceptable treatment in all pregnancy trimesters